26 yrs post partum female with headache
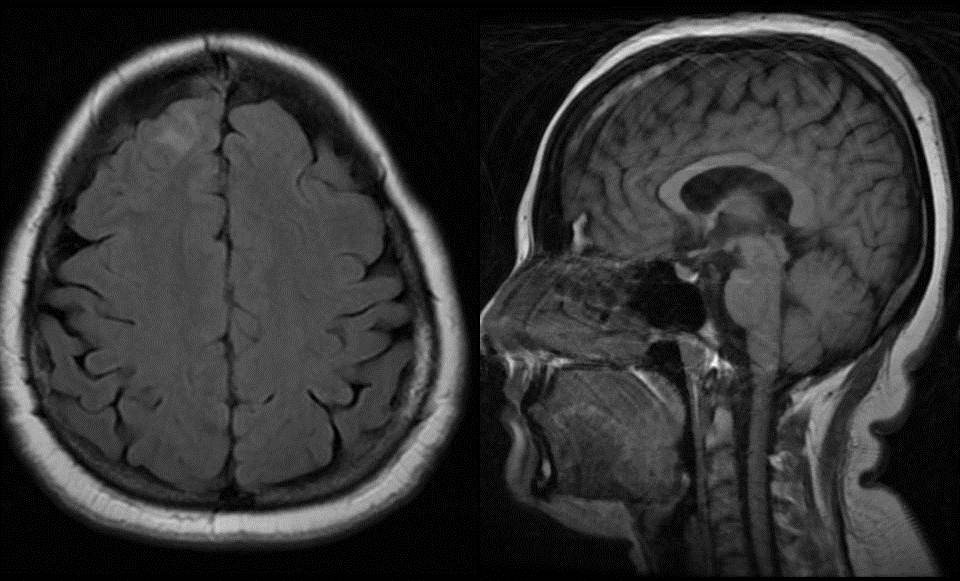 |
| Axial FLAIR and Mid sagittal T1 wt sequences: Mild FLAIR hyperintensity in right frontal cortical and subcortical region. Hyperintensity along the anterior aspect of superior sagittal sinus on T1. |
 |
| TOF MR venogram revealed thrombosis of anterior aspect of superior sagittal sinus. DWI revealed restricted cortical diffusion in right superior frontal gyrus- suggestive of acute venous infarct due to superior sagittal sinus thrombosis. |
Causal factors:
1. Local - sinus trauma, regional infection such as that in mastoiditis, and
neoplastic invasion or compression.
neoplastic invasion or compression.
2. Systemic- protein S and protein C deficiencies, peripartum state,
oral contraceptive use, and hypercoagulable states secondary to
malignancy.
oral contraceptive use, and hypercoagulable states secondary to
malignancy.
3. Unidentified – in 25%.
· Focal neurologic symptoms are more often seen in patients with
parenchymal changes observed at imaging than in those without such
changes.
parenchymal changes observed at imaging than in those without such
changes.
· The deep venous system drains the inferior frontal lobe, most of the deep
white matter of the frontal, temporal and parietal lobes, corpus callosum,
upper brainstem, basal ganglia and the thalamus.
white matter of the frontal, temporal and parietal lobes, corpus callosum,
upper brainstem, basal ganglia and the thalamus.
· Increased attenuation in the venous sinuses on CT also may be seen in
patients with dehydration, an elevated hematocrit level, or a subjacent
subarachnoid or subdural hemorrhage.
patients with dehydration, an elevated hematocrit level, or a subjacent
subarachnoid or subdural hemorrhage.
· In most cases, a close comparison of sinus attenuation with arterial
attenuation can help differentiate between a physiologic increase in sinus
attenuation and increased attenuation due to thrombosis.
attenuation can help differentiate between a physiologic increase in sinus
attenuation and increased attenuation due to thrombosis.
· Empty Delta Sign
· The signal intensity of venous thrombi on T1- and T2-weighted MR images
varies according to the interval between the onset of thrombus formation
and the time of imaging.
varies according to the interval between the onset of thrombus formation
and the time of imaging.
Stage of bleed/sequence
|
T1
|
T2
|
Acute
|
Iso
|
Hypo
|
Subacute
|
Hyper
|
Hyper
|
Chronic
|
Iso
|
Iso/Hyper
|
· Organized thrombus with intrinsic vascularity in chronic CSVT can enhance
with contrast.
with contrast.
· GRE imaging sequences may be an important diagnostic aid in
acute-stage thrombosis, when the signal intensities on
T1- and T2-weighted images may be more subtle.
acute-stage thrombosis, when the signal intensities on
T1- and T2-weighted images may be more subtle.
· DWI allows subclassification of parenchymal abnormalities
as either primarily vasogenic edema (with increased ADC values
presumably related to venous congestion) or primarily cytotoxic edema
(with decreased ADC values related to cellular energy disruption).
as either primarily vasogenic edema (with increased ADC values
presumably related to venous congestion) or primarily cytotoxic edema
(with decreased ADC values related to cellular energy disruption).
· Patients with diminished ADC values more often have parenchymal sequelae,
while those with normal or increased ADC values usually do not.
while those with normal or increased ADC values usually do not.
· In contrast with arterial ischemic states, many parenchymal abnormalities
secondary to venous occlusion are reversible.
secondary to venous occlusion are reversible.
· Parenchymal swelling without abnormalities in attenuation or signal intensity
on images may occur. Such patients typically have more prominent clinical
symptoms than would be expected on the basis of imaging findings.
on images may occur. Such patients typically have more prominent clinical
symptoms than would be expected on the basis of imaging findings.
· The enhancement is typically gyral in location and may extend into the white
matter.
matter.
· Increased tentorial enhancement (likely related to dural venous collaterals),
adjacent leptomeningeal enhancement, and prominent cortical venous
enhancement (secondary to venous congestion) also may be visible.
adjacent leptomeningeal enhancement, and prominent cortical venous
enhancement (secondary to venous congestion) also may be visible.
· Flame-shaped irregular zones of lobar hemorrhage in the parasagittal
frontal and parietal lobes are typical findings in patients with
superior sagittal sinus thrombosis.
frontal and parietal lobes are typical findings in patients with
superior sagittal sinus thrombosis.
· Hemorrhage in the temporal or occipital lobes is more typical of transverse
sinus occlusion.
sinus occlusion.
· Thalamic edema is the imaging hallmark of deep venous thrombosis and it
may extend into the caudate regions and deep white matter.
may extend into the caudate regions and deep white matter.
· “Cord sign ”and “Hyperintense vein sign ” are typically seen in isolated
cortical venous thrombosis on CT and MRI respectively.
cortical venous thrombosis on CT and MRI respectively.
· CSVT mimics
ü Sinus hypoplasia
ü Flow gaps
ü Arachnoid granulations
ü Thrombus shine signal
Ref: Imaging of Cerebral Venous Thrombosis: Current Techniques, Spectrum of Findings, and Diagnostic Pitfalls Radiographics
October 2006 26:suppl 1 S19-S41; doi:10.1148/rg.26si055174
Ref: Imaging of Cerebral Venous Thrombosis: Current Techniques, Spectrum of Findings, and Diagnostic Pitfalls Radiographics
October 2006 26:suppl 1 S19-S41; doi:10.1148/rg.26si055174
No comments:
Post a Comment
Please leave your comments